If you carry a firearm for personal defense, you do so because you recognize a basic reality: Should you find yourself the target of criminal violence it will be entirely up to you to protect yourself from the immediate danger. Bystanders are typically useless and police response will be too slow to do you any good. You are on your own. Most of us are probably pretty comfortable thinking about being on our own for the act of violence due to the lag time in police response, but what about dealing with an injury sustained in the struggle?
An excellent average response time from EMS would be about 5 minutes from the time the call goes out. A major arterial bleed can be fatal in 2-4 minutes. That means even excellent average EMS response time will be too late…and unfortunately there is no guarantee that EMS response time will be excellent. Consider the shooting in Aurora Colorado. Police were on scene and had the shooter in custody within a few minutes, but EMS response was delayed:
“On the police radio transmissions, officers said they lacked sufficient medical support for about 30 minutes after the 911 calls came flooding in around 12:39 a.m. and that medical teams didn’t report getting inside the theater for about 24 minutes. It wasn’t clear whether police efforts to secure the multiplex contributed to the delay in getting medical teams inside.”
Combine legitimate worries about more than one shooter, dispatchers swamped with 911 calls, poor communication and lack of coordination between police, fire, and EMS responders and you get this result. People died because of this delay, folks. Do not assume that once the bad man has been dealt with that EMS will be on scene immediately to help you. You’d best be prepared to do some things to help yourself.
The Tactical First Aid and “System Collapse” Medicine course offered by Active Response Training is aimed at giving the layman enough solid information to help them respond effectively to the sorts of wounds that happen in a combat environment. Penetrating trauma from bullets, knives, fragmentation from explosives, or even traumatic amputations from blast injuries aren’t terribly common in the United States therefore most of our first aid protocols and training don’t really take them into consideration. The US Military, on the other hand, deals with lots of penetrating trauma and has developed some extremely effective protocols and equipment to save people’s lives. Greg Ellifritz borrows heavily from the military’s protocols that have proven to be so effective at saving lives in the GWOT for this course.
Greg began class by breaking down an extensive DOD study on combat deaths and highlighting the types of injuries that could be helped with proper intervention. Some wounds are fatal and there’s no amount of intervention that’s going to help it…but careful study of the ways people died in combat found that the leading causes of preventable death were:
60% – bleeding to death from extremity wounds

33% – Tension pneumothorax
6% – airway obstruction
Greg rolls into class with a bunch of big plastic bins full of different types of tourniquets, pressure dressings, and various other goodies that you actually use under his supervision during the class. Each different type is pulled out and demonstrated. The strengths and weaknesses are discussed and then you have a go putting it on yourself and on a training partner. This may not seem revolutionary, but I’ve been through a couple of Red Cross classes before complete with certifications and I never once actually applied a pressure dressing…much less had the chance to try out all the major types of them to see which one I liked the best. (The OLAES and the Cinch-Tight are my faves, BTW…as for torniquets, I think the SOF-T is king of the hill. I bought 8 of them.) The ability go go hands on with this stuff and learn how to apply them efficiently beats the hell out of trying to read the printed instructions on the packaging while someone is bleeding out.
In addition to the commercial products Greg discusses ways to effectively improvise tourniquets and pressure dressings in a pinch. You learn the why in this class which helps you get a good handle on the how of doing something useful about it. Along the way a lot of tips and tricks are thrown in as well. It’s because of something Greg mentioned (“Sure, you know how to use this, but what if you are the one who is injured and someone else is trying to use your first aid kit to help you?”) that I’m keeping the instruction card for my SOF-T’s rubber-banded to the TQ itself just in case someone has to put one on me.
A great deal of time was spent discussing proper use of a tourniquet, (As high up on the bleeding limb as possible, never on a joint) including ways to convert an applied TQ to a pressure bandage to prevent any damage to the tissue downstream from the TQ in a situation where the casualty can’t get proper medical attention in a timely manner. A TQ can be left on a limb for 2 hours with no ill effects, and in most situations here in the United States that should be plenty of time to get someone to a hospital where they can get competent care. If you can’t get to a hospital within 2 hours conversion might be necessary. If a TQ has been on for 6 hours or more, it cannot be removed outside a hospital setting.
In addition to discussing TQ’s and pressure dressings, Greg explained the various hemostatic agents on the market. The most widely known probably being the granular Quick-Clot and Combat Gauze. Granular Quick Clot has been discontinued but there is still a bunch of it floating around out there, especially in military surplus medical kits. It’s pretty nasty stuff that, as Greg explained, basically boils away the liquid component of blood to leave only the bits of blood that will help form a clot. It’s certainly better than bleeding to death, but it causes intense heat and the wound it’s applied to has to be very carefully cleaned by surgeons afterwards. It’s also possible for small particles of it to end up floating around in the air getting in the eyes of the ones trying to help the casualty. Imagine the feeling of the moisture on your eye boiling for a second.
Combat gauze is gauze impregnated with a special type of clay that simply absorbs moisture, producing no heat and making no messes that surgeons have to clean up. It’s extremely effective and about the best you can do on a major bleed where you can’t apply a TQ. It’s also kind of expensive…but Greg happens to be an authorized dealer for the stuff and if you’re in one of his classes he’ll sell you some at cost.
…and all of that just barely touches on my notes from just the instruction on massive bleeding. Greg covered the rest of the MARC protocols (H was beyond the scope of 1 day of instruction) in the morning section at a quick pace that still allowed for a lot of hands on and questions. Again, this was intended to be enough information and exposure to give folks options for that period of time when they are on their own. It doesn’t make somebody an EMT or a doctor. It’s very targeted instruction aimed at helping someone take useful action to survive long enough to get into the hands of competent high-level medical intervention.
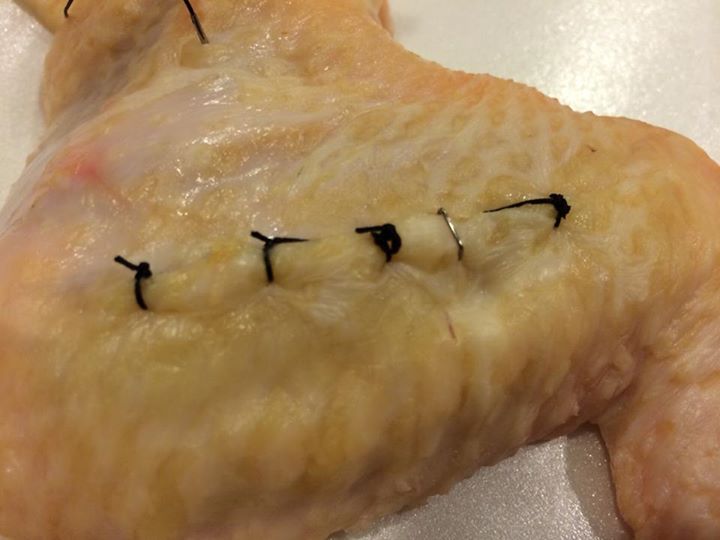
The “System Collapse” portion of the course was even more interesting as Greg explored the ramifications of a short term disruption in social order on medical support. Ebola is all over the news right now, but folks forget about events like Katrina when hospitals and ambulance crews were out of commission for quite some time. Riots, natural disasters, disease outbreaks, and acts of terrorism can place such a burden on our medical infrastructure that it may not be available for all of your needs. Greg likes to go to remote places of the globe where there is no medical infrastructure and has learned to keep himself (and others) alive and healthy without ready medical support on standby. He shares some of his strategies with his students, and even teaches them some of the skills he’s found useful. The highlight has to be going hands on applying sutures to a cut Greg made in some chicken wings. First the demo:
Then you get hands on with your own chicken. (Chicken skin is much thinner and more delicate than human skin) Never having stitched anything in my life, I was rather pleased with the results I got on my chicken wing.
The course throws a lot of information at you and good notes are essential for getting the most out of it…but I walked away retaining a lot of excellent information that I will hopefully never have to actually use. I’m a huge fan of training in general, but this kind of training should be at a much higher priority than it’s given by lots of folks in the gun world.
The world is not going to become a calmer place anytime soon, folks. With ebola all over the news and radical islamists carrying out individual acts of jihad it could well be you that’s able to make the difference if you have the right training and equipment. One man with hardly any formal training made the difference in several lives by applying improvised tourniquets in the immediate aftermath of the Boston bombing. The training you get in this course could be the thing that saves your life or the life of a loved one. If you’re able to get into this class with Greg or a similar class with another reputable instructor, do so with all speed.
Is there value in any decent training? Yes so not trying to knock this trainer or their courses!
But if you’re serious about medical training I’d suggest another approach. A person may do well to consider a first responder course for four reasons:!
1. It’s cheap ($200-300)
2. It local (I’ve never had to drive more than 20 miles for one so no flying or hotels to add to the cost/time commitment).
3. It’s long enough to do some good (40 hours broken up to fit real people’s schedules).
4. You’re training with the people who are likely to be the first on the scene if your brown smelly stuff hits one or more of the big whirling metal thingies. I personally find comfort in knowing the strengths and weaknesses of the medics… And myself (eye wounds give me a not nice feeling)!
Ok so once you’ve gotten a decent base of knowledge what then? Maybe look at a tactical medic course or some other training/gear as your budget allows.
An informative review and a good read. Thanks.
Are the preventable death statistics from a current (GWOT, OEF, OIF) DOD study or past (Vietnam)?
What matters is that the proper use of Tourniquets saves lives. With that said, I’m sure Caleb is going to stick one of his newly purchased TQ’s into his range bag along with some other “bleeder” gear and one into his hunting bag. As well as his car and EDC battle belt next to his speed loaders and Bowie knife.
As a firearms “enthusiast” I think there is a real possibility of seeing someone shot at an event, class, competition, hunt, anywhere there are a lot of people with guns… It would be nice to add value to the situation.
It’s also not a bad idea to keep a sharpie marker with that TQ to mark the time that it is applied – ER docs appreciate that. “Yeah doc I don’t know what happened, one minute my bromigo is lined up on this Boone and Crockett buck and the next thing I know he puts a 150gn Barnes TSX through his femur”. After your Bromigo wakes up and thanks you for saving his life you can laugh about writing what time the TQ was applied in permanent marker across his forehead.
KT